Cuban dares Democrats to run a hospital on Medicare rates alone — transparently, no subsidies — and then scale it. That experiment already has a name. He just described Medicare for All with the price tag showing.
Mark Cuban posted a dare this week. Take a small hospital, one of the many already circling the drain. Charge nothing but Medicare rates, for everything. Open the books to the penny so the country can see what it truly costs to run the place. Take no government money. Break even or fold. Do it once, then buy another, then another, until you have a network. He noted that some hospitals already manage this, so it wouldn’t even be novel. Then he closed with the tell: he tried, and the hospitals ghosted him the moment they learned how transparent he wanted to be.
It’s a good dare. I’ll take it. Every Democrat with a checkbook should take it. But Mark should understand what he’s actually asking us to build, because he has spent two years assembling the case that answers his own challenge, and the answer runs the opposite direction from the gotcha he thinks he’s holding.
Start with what he gets right, because he gets a lot right. The transparency demand is correct. Opacity is the load-bearing wall of the whole structure, which is exactly why the hospitals stopped returning his calls. The markup is real and he has documented it better than anyone with a microphone. He likes to ask why an insurer will pay $2,500 for an MRI when a center down the street will run the same scan for a few hundred dollars. That spread has nothing to do with the machine or the radiologist. It is the toll the system charges for walking through the more expensive door. He built Cost Plus Drugs to prove the same point one floor down: the price of a generic pill is the middleman, not the medicine. And he has said the quiet thing out loud — that everything in a hospital could cost a dollar and the insurers would still buy it, raise the price, and grow their margins anyway. That is a man telling you, plainly, that price in American healthcare has been pried loose from cost.
So here is my question back, Mark. If price has been pried loose from cost everywhere you’ve looked, why does your dare treat “what it truly costs to run a small hospital today” as if today’s costs are the true ones? They aren’t. Today’s costs are inflated by the same machine you keep indicting. You’re asking us to prove the rate works by running the test inside the very system that makes the rate look impossible.
That’s where the dare quietly rigs itself. A single Medicare-only hospital, taking no subsidies, surrounded by the current system, is not a clean experiment. It’s one boat ordered to stay dry in a flood. It still buys nurses, supplies, and machines in a market whose prices are set by competitors swimming in private overpayment. It still has to staff a 24/7 emergency room, treat everyone who walks in under EMTALA, and carry the unprofitable service lines — the psych beds, the rural OB unit, the standby capacity — that its cream-skimming neighbors are free to shed. And it’s denied the one trick every other hospital uses to survive: cost-shifting, charging the privately insured triple to cover the rest. Strip a hospital of the markup but leave it holding the whole region’s dumped costs, and of course the books look ugly. That ugliness isn’t a verdict on Medicare rates. It’s a snapshot of what the system does to anyone who tries to step out of it alone.
Now look at the examples Cuban offers as proof it can be done, because both of them argue for the other side. Cash surgery centers do thrive at Medicare rates and below — the Surgery Center of Oklahoma model prices procedures at roughly half what Medicare pays the big hospital systems, a tonsillectomy for under four thousand dollars against a seventy-two-thousand-dollar hospital quote. But they pull it off by handling the schedulable, elective, shoppable work and refusing the rest. They prove the rate is plenty for the care delivered. They do not prove a full-service hospital can break even as an island, because they aren’t full-service hospitals. And the rural hospitals Cuban points to “surviving on Medicare”? They survive because Medicare pays Critical Access Hospitals 101 percent of their reasonable costs instead of the standard fixed rates, a deliberate cost-plus carve-out precisely because low-volume hospitals cannot live on standard Medicare rates. His own example is a federal admission that the standard rate runs below cost for thin-volume facilities, and that the fix is to pay cost. Rural health analysts have made the next move explicit: if every payer reimbursed at cost the way Medicare does for these hospitals, many of them would turn profitable. That is the single-payer argument wearing work boots.
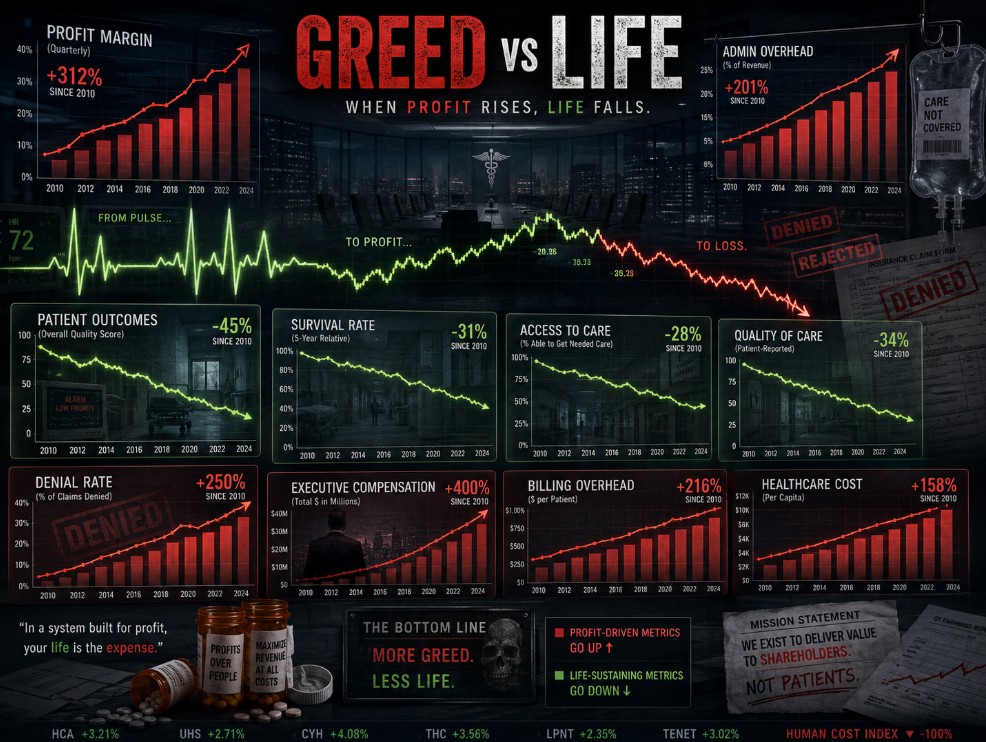
This is the whole case in one line. The gap between Medicare rates and “what it costs” is not the price of healing people. It’s the price of competing for insured ones. It’s the duplicate cath labs in three hospitals that each need one, the marketing budgets, the chargemaster theater, and above all the billing army required to fight a hundred payers at once. Administrative overhead runs about 34 percent of US health spending, on the order of 1.7 trillion dollars a year. The Yale study Cuban waves off doesn’t conjure its savings from thin air; it finds them right here, crediting around 219 billion in administrative savings plus another 35 billion a year hospitals burn just chasing unpaid bills, for a total 13 percent cut to national health spending, more than 450 billion a year. Pull the maze, and the rate covers the care. That has always been the premise.
Which brings us to the staircase Cuban drew himself. One hospital, then another, then a network. Mark, that’s not a dare. That’s a blueprint. Every Medicare-only hospital that opts out of cost-shifting and cream-skimming is a small single-payer island, and a chain of them stitched together is the Yale result reconstructed building by building. The reason one island bleeds and the network thrives is the entire point: the inefficiency is systemic, so the cure has to be too. You can’t fix a flood one dry boat at a time.
I’ll even concede the part you’d crow about. Run that first hospital honestly, no subsidies, today, and the early books would be brutal. It might not clear break-even in year one. But the bleed would be the diagnosis, not the rate — the cost of being surrounded. Give it the conditions Khanna’s pilots are reaching toward — every payer at cost, no cream-skimming next door, capacity rationalized instead of duplicated — and it clears break-even with room to spare. The national math says thirteen percent of room.
So yes. Let’s take the dare. Let’s open the books to the penny, exactly as you asked, because transparency was never my enemy. Let it show what the spread really pays for. And when it does, let’s stop calling the answer a dare and start calling it what it is, a network.